
Equestrian sport is unusual among Olympic disciplines: it is sex-integrated, participation spans decades, and many riders remain competitive well into midlife and beyond. That longevity is a strength—but it also means that a large proportion of the riding population will experience perimenopause and menopause while still training, competing, coaching, and caring for horses. In other sports, the menopause transition is increasingly recognised as a performance and wellbeing issue. In equestrianism, until very recently, it has been largely invisible in research, coach education, and everyday stable-yard conversations.
My research set out to make that “hidden middle” visible: to document how perimenopause and menopause are perceived to affect riding participation and performance, to identify the challenges riders report, and to consider what coaches and support networks can do differently. It was conceived based on my own personal lived experience and further by the observations and conversations with saddle fitting and coaching clients.

WHY THIS MATTERS IN EQUESTRIANISM SPECIFICALLY
At performance level, success in equestrian sport depends on more than physical capacity: it rests on attention, emotional regulation, decision-making under pressure, confidence, and a responsive partnership with a horse. Riders describe elite performance as requiring confidence and anxiety control—traits that can be disrupted by sleep disturbance, mood fluctuation, anxiety, cognitive “fog,” pain, fatigue, and thermoregulatory changes commonly reported during the menopausal transition.
In other words: even when perimenopause doesn’t stop someone riding outright, it can alter how safe riding feels, how quickly skills consolidate, how resilient a rider feels to criticism, and whether training and competing still feel enjoyable. When the sport also involves risk (falls, speed, jumping, cross-country), a shift in confidence or recovery capacity can change behaviour quickly—sometimes in ways that are misread as “lack of commitment” or “loss of edge,” rather than a rational adaptation to a new embodied reality.
STUDY OVERVIEW: CAPTURING LIVED REALITIES AT SCALE
The study recruited 1,629 female equestrians from a broad range of disciplines, aged 21–73 (mean age 51.86 ± 14.95), who believed they were within or beyond perimenopause/menopause.
While the sample is self-selecting (and therefore not a prevalence study of “how many riders have symptoms”), its scale provides something the equestrian sector rarely has: a wide-angle view of the issues riders themselves consider most disruptive, alongside direct accounts of what those disruptions feel like in day-to-day riding life.
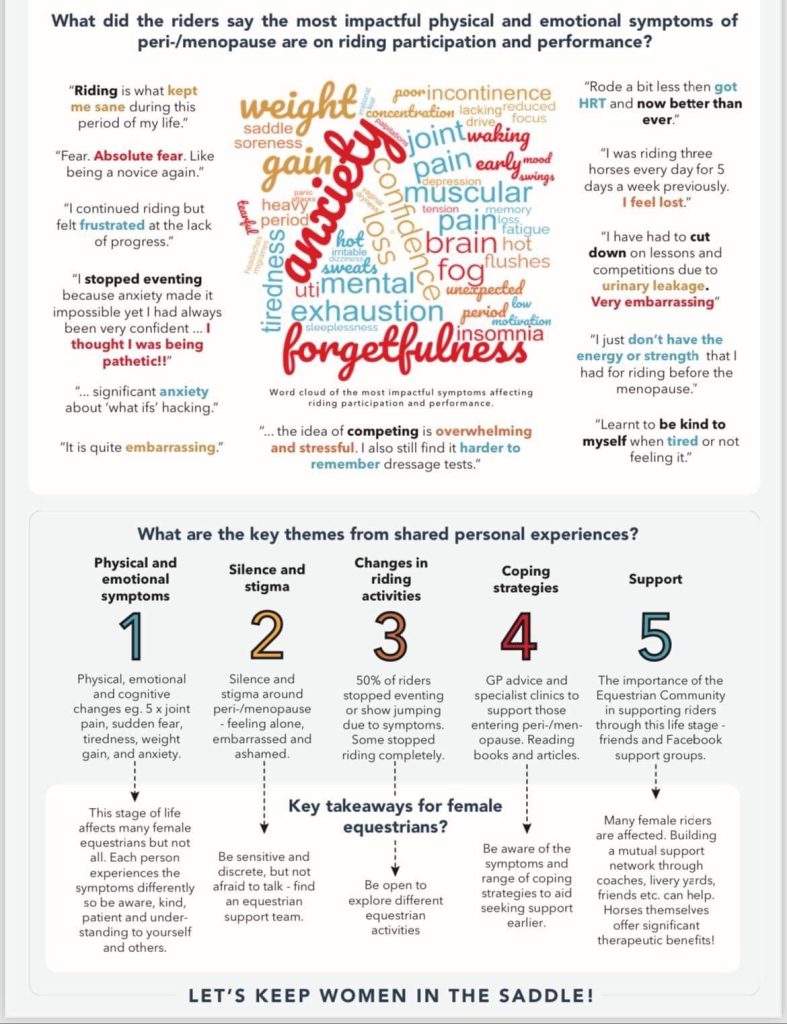
WHAT RIDERS REPORTED: THE SYMPTOM CLUSTER THAT HITS RIDING HARDEST
Across the dataset, riders repeatedly identified a cluster of physical, psychological, and cognitive symptoms that interfered with both participation and performance. The most prevalent symptoms included:
- Joint pain (74%), decreased physical strength (71%), weight gain (66%)
- Sleeplessness (74%), anxiety (78%), loss of confidence (76%)
These numbers matter because riding performance is not solely determined by skill; it is mediated by comfort in the saddle, capacity to absorb physical load (mounting, yard tasks, core/postural endurance), and readiness to make rapid decisions. Chronic sleep disruption and anxiety also have well-established links to cognitive performance—attention, working memory, and the “sharpness” riders often describe as necessary for timing and feel.
The riders’ own words brought those statistics to life. They described:
- embarrassment and withdrawal linked to symptoms such as urinary leakage or unpredictable bleeding;
- heat intolerance and exhaustion affecting training and competition;
- “brain fog” and forgetfulness affecting recall of dressage tests;
- reduced robustness to criticism (even when constructive), changing who they felt able to train with, or stopping completely.
This is a key coaching insight: perimenopause doesn’t only change the rider’s body—it can change the coach–rider relationship, because it changes what feels tolerable, what feels threatening, and what feels like a “good session.”
CONFIDENCE, RISK, & THE RESHAPING OF RIDING IDENTITY

A standout finding was the extent to which riders described confidence loss and risk recalibration. For many riders, confidence shifts were one of the most immediate and costly changes.
A huge 75% reported a decrease in riding confidence, particularly around faster work, jumping, and fears of injury or longer healing time. Participation in higher-risk disciplines shifted markedly: showjumping and eventing participation reduced by around half, with riders moving to “less risky” activities, reducing intensity, or stopping altogether.
This matters because identity in equestrian sport is often discipline-linked (“I’m an eventer”, “I’m a showjumper”). When a rider adapts discipline due to symptoms, the change can feel like a loss of self, not just a training modification. Coaches who interpret this as a motivation issue may inadvertently deepen the rupture, whereas coaches who name it as an adaptation can protect both confidence and continuity.
PARTICIPATION & ENJOYMENT: WHEN RIDING STOPS FEELING LIKE AN OUTLET

A significant proportion of respondents reported reduced enjoyment and changes to participation. Four riders in five reported reduced enjoyment, and around a third reported stopping riding completely, temporarily, or adapting their activity.
For many women, riding is not only sport but also stress relief, community, and identity. When symptoms push them out of the saddle, the loss can be psychologically significant—particularly when it happens alongside other midlife transitions (workload, caregiving, changing body image). This provides a strong rationale for treating perimenopause awareness as a retention and wellbeing issue for the whole equestrian industry, not a niche health topic.
COACHING DISRUPTION: THE QUIET COLLAPSE OF THE TRAINING RELATIONSHIP
One of the most practically important (and arguably most worrying) findings concerns coaching access and openness.
- Over 62% of riders reported stopping coaching sessions permanently or temporarily.
- Of those who continued coaching, 60% said sessions were negatively impacted by peri/menopause symptoms.
- Only 50% felt able to speak openly to a female coach, and just 10% to a male coach about issues affecting their riding.
This is not just about “awkward conversations.” It suggests that the very mechanism that could support adaptation—coaching—is often the first thing riders withdraw from, exactly when they need sensitive progression, safety planning, and reassurance.
Why do riders stop coaching? The qualitative comments imply multiple drivers: embarrassment about symptoms, fear of being judged, reduced energy for structured sessions, lowered tolerance for critique, and a lack of confidence that the coach will respond with empathy.
SILENCE & STIGMA: THE SOCIAL CONTEXT THAT SHAPES SYMPTOM IMPACT
The study also points to silence and stigma as a theme in itself. Riders described feeling alone, embarrassed, or ashamed—particularly around symptoms that are culturally coded as “private” (bleeding changes, urinary leakage, mood volatility). This matters because stigma magnifies impact: it increases avoidance (of coaching, of competing, of asking for help) and reduces the likelihood of reasonable adaptations being made early.
From a systems perspective, silence also blocks learning. If coaches rarely hear what riders are managing, coach education remains focused on technical progression and misses a major barrier to sustained participation for a large portion of the riding population.

COPING STRATEGIES & SUPPORT: WHAT HELPED (& WHAT DIDN’T)
Riders reported a range of coping strategies, including seeking GP advice, using specialist clinics, reading and learning, and leaning on friendship networks and online support groups.
Hormone Replacement Therapy (HRT) emerged as beneficial for many riders, alleviating symptoms that interfered with riding and daily life—though experiences of accessing effective support through primary care were mixed, with some reporting better outcomes via specialist menopause clinics.
It’s important to be clear: this research does not claim HRT is “the solution,” nor does it provide medical guidance. What it shows is that symptom relief—however achieved—can restore capacity, confidence, and enjoyment, and that signposting and normalising help-seeking may be an important role for coaches and organisations.
Recent announcements from the U.S. Food and Drug Administration indicate a significant shift in how hormone replacement therapy (HRT) is being viewed. The FDA has publicly acknowledged that earlier risk-averse categorisation of HRT was based on flawed and incomplete evidence, and that for many women, HRT represents a more clinically appropriate and effective treatment for menopausal symptoms than alternatives such as antidepressants for hormonally mediated low mood, or repeated antibiotic use for menopause-related urinary tract symptoms.
This recalibration in medical thinking has yet to be fully reflected in UK clinical practice. Many general practitioners continue to base advice on outdated interpretations of the evidence, mirroring the position previously held by the FDA. As a result, women are often required to advocate strongly for themselves and would benefit from attending GP consultations armed with current, evidence-based information.
Louise Newson, a leading UK menopause specialist and long-standing advocate for informed patient choice, has played a prominent role in improving awareness and access to evidence-based menopause care. However, her work was subject to controversial and, many argue, misrepresented criticism in a Panorama documentary, which presented an imbalanced narrative and sensationalised concerns around HRT prescribing. The programme implied opportunistic over-prescription and exaggerated risk, contributing to public confusion rather than informed debate.
Taken together, these issues highlight how far there remains to go in the UK to rebalance menopause care, align clinical guidance with contemporary evidence, and move beyond legacy narratives that continue to shape both professional practice and public perception.
PRACTICAL RECOMMENDATION TO COACHES TO “KEEP WOMEN IN THE SADDLE”

- Be aware of symptoms; be kind, patient, and understanding.
This is not a call to lower standards; it is a call to coach the human in front of you. If sleep has collapsed and anxiety is high, a rider may need different cue density, pacing, and goals that day. - Be sensitive and discreet.
Avoid public calling-out. Offer privacy for conversations. Let riders choose what to disclose. - Be flexible with coaching plans “on the day.”
Build optionality: alternatives to jumping, shorter blocks, more recovery, different warm-ups, or confidence rebuilding exercises when symptoms flare. - Support and encourage changed activities (without shaming the shift).
If an eventer moves to dressage for a period, frame it as a tactical adaptation, not a retreat. Protect identity and self-efficacy. - Sensitively signpost to relevant support networks.
Coaches are not clinicians—but they can normalise help-seeking, recommend reputable education resources, and encourage riders to speak to healthcare professionals.
A useful coaching mindset here is curiosity over judgement. When a rider’s behaviour changes—avoidance, irritability, hesitation, withdrawal—the question is not “what’s wrong with her commitment?” but “what’s changing in her capacity, confidence, or comfort, and what adaptation would keep her riding safely?”
WHAT THIS MEANS FOR THE INDUSTRY
Because equestrian sport depends so heavily on adult female participation (as riders, owners, volunteers, officials, and consumers), the menopausal transition is not a fringe issue—it is a participation and sustainability issue. The data suggest that large numbers of riders reduce activity, stop coaching, or step back from higher-risk disciplines during perimenopause/menopause.
That creates a clear call to action for national governing bodies, clubs, yards, and coach education providers:
- embed menopause/perimenopause awareness into coach training,
- improve the psychological safety of coach–rider communication,
- create visible pathways for support and signposting,
- and treat midlife retention as strategically important—not incidental.
CLOSING THOUGHT

Perimenopause is not simply a biological event; in equestrian sport it becomes a performance, confidence, identity, and relationship issue—often managed in silence. I hope my research shows that the impacts riders report are real, multi-dimensional, and frequently strong enough to change behaviour, participation, and coaching engagement.
If we want to “keep women in the saddle,” the answer is not to tell riders to push through. It is to build a culture that recognises this life stage, makes space for honest conversation, to seek hormonal advice from knowledgeable medical professionals, and adapts training in ways that protect both safety and sporting joy—so that experience and talent are not lost at the point they should be most valuable.

🌐 http//:www.freedomsaddlery.co.uk

